

Serving patients and family members on Alzheimer’s disease and aging with a holistic approach, Acıbadem Healthcare Group uses neurologic and psychiatric examinations, dietician and psychologist consultations and neuropsychological tests to ensure early diagnosis and appropriate treatment plan for Alzheimer’s disease.
Diagnosis and Treatment Services for Alzheimer’s Disease and Aging
The patients are assessed by neurologists and psychiatrists regarding treatment of Alzheimer’s disease; early diagnosis, medical follow-up, medical and social rehabilitations are carried out following a process consisting of various blood tests, urinalysis, MRI, EEG and neuropsychological tests.
The risk of disease is analyzed for people with family history of Alzheimer’s disease. People who are at risk are informed about prevention of the disease and they are followed up on a regular basis.
Diagnosis of Alzheimer’s Disease and Diagnostic Tests
Physician:Obtains medical history from the patient and family members.
Confirms the key finding stated by patient and/or the family member.
A screening test is performed to verify presence of dementia. The widely acknowledged screening test is Mini Mental State Exam (MMSE). This test examines time and place orientation, learning, numerical problem solving, remembering, labeling, sentence writing and visual memory of the patient. Mini Mental State Exam (MMSE) was first used in 1975 by Folstein and colleagues.
The test aims quantitative evaluation of impairment in memory and other areas. It addresses if the patient answers questions correctly and cooperates with commands. It cannot diagnose dementia, but it provides details about whether there is cognitive impairment or not. Next, other tests are also done by neuropsychologists.
Neuropsychological TestsA psychologist orders detailed neuropsychological tests to verify the core finding and determine other intellectual losses according to the result of screening test – mostly Mini Mental State Exam – to establish diagnosis of Alzheimer’s disease. Neuropsychological tests are a battery of examinations that provide tangible data on memory, daily life and behaviors.
Psychologist chooses a test according to native language and educational status of the patient. While some of the tests are completed and results are reported within very short time, others may require some time to get more detailed information.
Neurophysiologic ExaminationsNeurophysiologic examinations are crucial for differential diagnosis of certain diseases. The most critical neurophysiologic examination is EEG (electroencephalography). As it reveals out extremely typical signs in certain types of dementia, such as Creutzfeld Jakop disease, it allows diagnosis within a very short period of time.
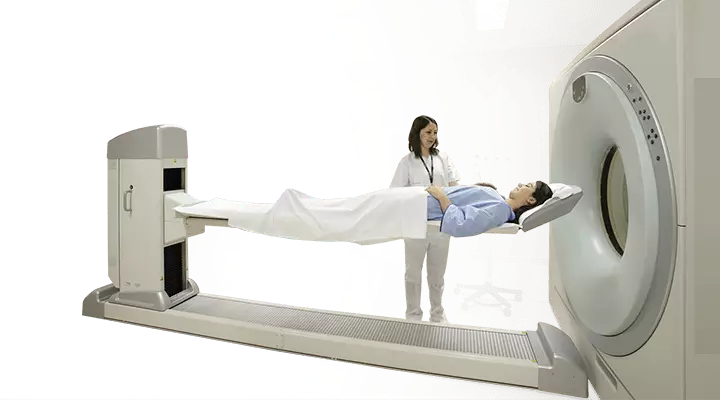
Radiology StudiesComputerized Tomography (CT) or Magnetic Resonance Imaging (MRI) can be scanned by radiologist to visualize involved areas of the brain. Volumetric or functional MRI can, sometimes, be scanned to calculate the lost volume in the involved part of the brain or to determine if a certain area of brain functions properly.
Nuclear Medicine ExaminationsRecently, nuclear medicine techniques gained importance to identify the metabolism of brain functions in routine daily life and during a disease, such as dementia, and to observe accumulation of amyloid protein, which is responsible for development of Alzheimer’s disease, many years before the onset.
These techniques are reserved for advanced stages of the disease due to their cost. However, amyloid-PET scan is valuable for the early diagnosis of disease and it is performed by Nuclear Medicine Specialists.
Clock Drawing TestClock drawing test is another screening method. Patients are asked to draw a clock, place the numbers and mark the instructed time. Geometrical skill (constructional praxis) of a person provides valuable information regarding the comprehension and planning capability.
Genetic and Laboratory TestsGenetics/Biochemistry/Hematology/Microbiology
These tests help differential diagnosis and they are analyzed to provide patients with certain genetic details. Thyroid hormones, Vitamin B12-Folic Acid, Glucose measurement, hemoglobin and other complete blood count parameters, erythrocyte sedimentation rate, electrolytes, urea and hepatic function tests are necessarily analyzed.
HIV and Syphilis should be assessed to rule out some infectious diseases. APO E epsilon 4 level can be measured. 14-3-3 protein should be analyzed in cerebrospinal fluid for diagnosis of Creutzfeld Jacob disease.
It is known that early diagnosis is possible for Alzheimer’s disease. Biomarkers imply proteins that are measured in cerebrospinal fluid of patients and known to cause the disease in order to diagnose the disease early.
These biomarkers may be analyzed in blood, but accurate and correct result can only be obtained from the analysis of cerebrospinal fluid. Studies show that these proteins start to elevate 20-30 years before onset of the disease.
These proteins, which can also be analyzed in our country, also allow early preventive measures against the disease.
Bio-markers used for early diagnosis of Alzheimer’s disease are total tau, phosphorylated tau, Ab42-Ab40 and BACE (beta secretase enzyme). Normal and abnormal ranges of these bio-markers may vary between laboratories.
Alzheimer’s disease is an irreversible disorder and has no certain cure. Medication treatment of Alzheimer’s disease aims alleviation of symptoms and treatment of co-existing disorders.
In addition, recovery of mental capacity and facilitating daily life are aimed.
Various medications have been developed in accordance with some theories regarding the cause of disease. When brain tissues are lost due to Alzheimer’s disease, level of acetylcholine – a substance responsible for learning – decreases, while concentration of glutamate increases which is a cause of serious inflammation and degeneration.
The existing drugs try to increase level of acetylcholine, while they act to decrease concentration of glutamate. Donapezil, Rivastigmine, Galantamine and Memantine are advertised brand names of drugs used for this purpose.
Side effects are followed up, after use of these drugs is started. If there is recovery, the drug is maintained without any change, or otherwise, either dose is increased or patient is switched to another drug.
Other Adjunct Treatments
Physicians may combine medical treatment with behavioral therapy, physiotherapy, ergotherapy, memory therapy, reality guidance (person, place and time orientation), biography and remembering, music, sense, aromatherapy and pet therapy.
Studies on novel treatments given to help patients regain health focus on preventing production and deposition of beta-amyloid and tau proteins that impair functions of neurons in brain and invention of drugs that accelerate conversion and excretion of such proteins, if they have been already synthesized.
It is planned to develop a vaccine against Alzheimer’s disease at further phases.
In conclusion, treatment of Alzheimer’s disease should cover;- Medication therapy
- Psychological support
- Exercise
- Nutrition.
Mediterranean diet has positive effects on the course of Alzheimer’s disease. Mediterranean diet encourages high consumption of herbal foods rich in fiber (vegetables, fruits, dry legumes, whole wheat), fish and olive oil and low amount of red meat, chicken, low-fat milk and dairy products.
Consumption of refined and sugar-added foods eases progression of the disease.
Milk and dairy productsMilk and dairy products, such as cheese, cottage cheese, curd and yoghurt, should necessarily be included in daily diet. This group of foods contains protein, calcium, phosphorus and Vitamin B and thus, it is beneficial to consume 2-3 servings a day.
Meat, dry legumes, egg and oil seedsRed meat, chicken, turkey, fish, egg, chickpea, white beans, green lentil and oil seeds, such as walnut, almond and hazelnut, fall into this group and they can all be used interchangeably. This group covers minerals, such as iron, zinc and magnesium, and vitamins A and E along with protein.
Fats and oilsConsumption of fats and oils should be limited, as we grow older. Animal fat and foods that contain animal fat should be avoided. As meat and meat products are very rich in saturated fat, fat-free ones should be preferred to consume these foods.
Extra virgin olive oil, avocado oil and canola oil should be preferred over sunflower oil. Moreover, fried foods should not be preferred, as they cause too much fat intake. Steaming or baking should be used for cooking instead of frying.
Omega -3Foods that are rich in omega-3 fatty acid are fish (fatty fish like sardine, salmon and mackerel), walnut and flaxseed. Sufficient omega-3 intake reduces risk of Alzheimer’s Disease. We recommend eating fish twice of three times a week to consume sufficient amount of omega-3.
Vegetable and fruitVitamins C and E in fresh vegetables and fruits decrease the risk of Alzheimer’s disease. Vitamin E is a fat soluble vitamin with antioxidative features. We should make room for raw almond, sunflower seed, olive, extra virgin olive oil, avocado and spinach that are rich in Vitamin E, which is a fat-soluble vitamin.
Vitamin C is a water-soluble vitamin; therefore, it is not stored in body and should be taken every day. It is beneficial to eat strawberry, broccoli, bell pepper, kiwi, melon, cauliflower, broad bean, blueberry, rose hip, raspberry and blackberry every day, as they are rich in Vitamin C.
Grains and grain productsWhole wheat bread, pasta, cracked wheat (bulgur), noodle and ground wheat are in this group. This group is our basic source of energy. Whole grain cereals and cracked wheat (bulgur) are rich in vitamin B. They play an important role in functioning of digestive and nervous systems. Soup should be particularly consumed in every meal.
SAMPLE MENUBefore breakfast: 1 glass of water
Breakfast- 1 glass of milk
- 1 thin slice of white cheese
- One boiled egg (2-3 times a week)
- 5 olives or half an avocado
- Tomato - cucumber - green pepper
- 1-2 slice(s) of whole wheat bread
1 serving of fresh fruit
Lunch- 1 bowl of soup
- Grilled fish, 200 g
- Season salad (2 dessert spoons of olive oil).
- 1 slice of whole wheat bread
1 serving of fresh fruit + 3 whole walnuts
Dinner- 1 bowl of soup
- 1 serving of vegetable meal cooked with olive oil
- 1 bowl of yoghurt
- 2 tablespoons of cracked wheat (bulgur) pilaf
- 1 slice of whole wheat bread
Psychological Support for Family Members of Patients with Alzheimer's Disease
The fact that any one of loved relatives or family members is diagnosed with Alzheimer’s disease is hard to accept. Behavioral and personality changes of the patient secondary to the disease boost concerns of family members and loved ones. Concerns about the disease may cause future anxiety for patients’ relatives.
A sad, worrisome and wearing treatment process begins for patients’ relatives following diagnosis of Alzheimer’s disease. Serious anxiety, internal conflicts and trying to suppress them may affect psychological health of family members.
Depression, anxiety disorder or stress related disorders are likely in family members or loved ones of patients. Therefore, relatives of patients with Alzheimer’s disease are recommended not to neglect themselves and start getting psychological support.
Advices for Family Members and Loved Ones of Patients with Alzheimer’s DiseaseAlzheimer’s disease is a progressive neurological disorder that causes loss of cognitive functions. Quality of daily life starts to impair at the onset of disease. Patients with Alzheimer’s disease have difficulty communicating with other people and fulfilling daily activities.
Serious personality and memory changes are recognized by family members, friends and colleagues. Patient starts to act abnormally at the onset of disease. Sleep cycle and diet of patients with Alzheimer’s disease start to be affected seriously.
Patients start to face difficulty shopping and managing their finances. Mood swings at frequent intervals are accompanied by sensitivity, depressive behaviors and tearfulness.
How Should Relatives Communicate with Patients with Alzheimer’s Disease?While communicating with patients, they should speak calmly and gently. A patronizing style of communication should be avoided. Short and understandable sentences are encouraged. Try using the word “please” a lot while talking to your patient.
Offering two choices in any subject will help the communication with your patient.
Memory impairments may cause your patient to deviate from realities and remember the names wrong. Patients’ relatives should not try to change their thoughts in such cases. Trying to correct the wrong thoughts may provoke distress. Instead, joining the patient’s perception can make him/her happy.
How Should Patients’ Relatives Handle Difficult Conditions Like Aggression, Bursts of Anger and Anxiety EpisodesWhile dealing with difficult situations, try to select affirmative, reassuring sentences with a calm tone. In cases of crisis, acting angry or feeling fear may complicate the efforts to cope with the crisis.
Especially in aggression and anger episodes, patients’ relatives should not allow the patient understand that they are frightened and concerned. Aggressive behaviors may worsen, if the patient recognizes them.
Similarly, anger of family members, caregivers or loved ones will provoke aggressive behaviors of patients. Therefore, patients should be approached in a cautious manner by selecting reassuring words and leaving a certain distance in case of physical attacks. Physical intervention to patient is not an accurate approach.
In case of a physical attack, you can use sentences like “please, you hurt me”.
Try to determine the conditions that induce aggressive behaviors. You can try to leave the room, until your patient calms down. You can try to guide your patient’s attention. For example, you can ask “shall we drink coffee together?” Ask for your doctor’s help if you lose control.
Accept unrealistic thoughts of your patient that he/she tries to explain in an anxiety episode. Try to talk with a calm voice and do empathy.
Try to convince your patient to do an activity that he/she is interested in, but do not insist too much. If your patient’s anxiety worsens substantially despite your empathy according to his/her perception at that time, contact your physician.
Alzheimer’s Disease
Alzheimer’s disease is a disorder of advanced age and it is manifested by memory impairment and dysfunction in all intellectual activities, daily activities and behaviors due to gradual damage to certain parts of the brain over time.
Alzheimer’s Disease is a condition of advanced age and number of patients with the disease is constantly increasing. The underlying cause is the aging population of the world.
The increase in figures of elderly population is primarily caused by decline in younger population and increased life expectancy at birth due to success of prevention methods developed against certain diseases that often cause death, such as cancer and cardiovascular diseases.
“Baby boom” implies the increased fertility rate in the United States of America and Europe in 1950’s following Second World War. This generation with higher population than previous ones has given birth to fewer children and the population has started aging faster than ever, starting in 2000’s.
Currently, there are approximately 40 million patients with documented Alzheimer’s disease, while it is estimated that the figure will be 115 million in 2050. Recent estimations assume that there are 600 thousand to 1 million patients in Turkey and it is believed that Turkey will be the 4th country around the world in terms of number of patients with Alzheimer’s Disease.
Early diagnosis and disease control at early stage are crucial that can be achieved by raising awareness on the disease. This approach increases quality of life not only for patients with Alzheimer’s Disease, but also for their relatives, while treatment costs are also reduced.
History of Alzheimer’s Disease
The disease was first described by Alois Alzheimer, a German neuropsychiatrist. Auguste Deter, 51, was brought to Dr. Alzheimer by the patient’s spouse due to progressive memory impairment and behavioral disorder in 1902. Dr. Alzheimer examined and followed up the patient until the patient's death in 1906 and performed an autopsy.
He saw thinned cortex and unusual accumulations in and around the cells in brain samples of the patient. After plaques and fibers were described, Alzheimer’s discovery was subsequently presented in medical conferences and the condition was named Alzheimer’s Disease.
Symptoms of Alzheimer’s Disease
Symptoms of Alzheimer’s Disease are as follows:Impaired MemoryImpaired memory is the first and the most important sign. Patients with Alzheimer’s Disease forget recent events, people and other details. Memory impairments worse and the patient cannot remember such details, as the disease progresses.
Impaired memory is characterized by simple forgetfulness episodes at the initial stages of the disease.
- Losing keys
- Forgetting the names
- Neglecting appointments
- Forgetting the change while shopping
- Leaving the stove on
- Memory impairment worsens in subsequent periods.
- Confusing the way to home and locations of rooms
- Confusing son with father and daughter with mother
- Adding sugar to food instead of salt
- Hiding money somewhere and inability to find it
- Difficulty in daily activities
Another key feature of the disease is trouble in activities of daily life. Most patients cannot plan out their daily chores and experience difficulty completing them. Sequential activities become challenging, such as cooking, choosing clothes or talking on the phone.
Patients lose acquired skills. They cannot knit, drive nails, cook, play instruments, go to bathroom, bathe/shower or eat. Enuresis and encopresis are likely or they void or defecate at unusual parts of home.
Psychiatric and Behavioral DisordersBehavioral and psychiatric symptoms, although existing since initial stages of the disease, are the prominent sources of struggle in the advanced stages.
Sudden-onset mood swings with no clear cause are likely in Alzheimer’s disease; they may cry easily, become withdrawn or get angry suddenly and inordinately. They become insomniacs, constantly move, wander, hallucinate, talk to mirrors, eat constantly or not at all, become skeptical, hide belongings and yell.
Behavioral disorders are the primary factors that make patients dependent on caregivers.
Other SymptomsLanguage impairments: patients may experience difficulty finding the right vocabulary or verbal fluency can be lost. The patient may use descriptions instead of words. It may, sometimes, be difficult to understand what the patient says and writes. For example, they may say “I use it to shape my hair” instead of comb. They can say they draw on paper with it instead of pen or pencil. They may make up words, saying “batle" instead of table.Confusing place and time: Patients with Alzheimer’s disease may confuse days, months and even seasons.They may get lost in familiar places, such as quarter of home, forget where they are or may not remember why they are there. The most common symptoms are forgetting stores, frequently visited mosques, workplace of many years, rooms of home, the day, hour of the day and months.
Perception of images may also confuse and disorders occur in reading and comprehension of shapes. Images may be confused with previously visited locations. They may confuse human faces. They may experience problems in traffic.
Problems in Judgment and Decision: They may experience difficulty choosing and deciding on foods and clothes. They may rug up or wear socks in different colors.Difficulty in Abstract Thinking: They confuse interpretation and meanings of proverbs. For example, when asked the meaning of little strokes fell great oaks, they may answer “water runs out of tap and fills in a container”.Misplacing possessions; Patients with Alzheimer’s disease can misplace objects or put them at unusual places. For example, they may place shoes in the fridge and keep eggs under beds.
Diagnosis of Alzheimer’s Disease According to DSM-V
DSM-V (Diagnostic and Statistical Manual of Mental Disorders) is a guideline that updates diagnostic criteria for mental disorders. In the light of scientific and most recently acknowledged data, following conditions should be met to diagnose dementia caused by Alzheimer’s disease according to DSM-V.
1. Dysfunction in tasks requiring complex attention
2. Dysfunction in executive tasks
3. Disrupted learning and impaired memory
4. Language impairment
5. Impaired perception
6. Disrupted social cognition
Diagnosis of Alzheimer’s Disease According to Alzheimer’s AssociationAlzheimer’s Association has released 10 symptoms, which are required to be known to clarify whether a person or his/her family members has/have Alzheimer’s disease. Having one or more of these symptoms require a visit to a relevant facility or a doctor.
1. Impaired memory that affects daily routines
2. Difficulty in planning and calculation
3. Inability to perform once-routine tasks
4. Confusing time and place
5. Difficulty comprehending images
6. Impaired speech and comprehension
7. Losing possessions and blaming others
8. Difficulty making judgments and decisions
9. Withdrawing from social activities
10. Changes in personality and behavior
Stages of Alzheimer’s Disease
Stages of Alzheimer’s Disease are defined by studies conducted in 2011:
1. Stage 1: No symptom is noticed (Preclinical)
2. Stage 2: Mild Cognitive Impairment
3. Stage 3: Mild Dementia
4. Stage 4: Moderate dementia
5. Stage 5: Moderate - Severe Dementia
6. Stage 6: Severe dementia
7. Stage 7: Very severe dementia
Stage 1 occurs much earlier before being noticed by the patient or a physician. Grades 2 and 3 can be combined to define mild cognitive impairment.
Preclinical Stage: Pre-clinical stage is characterized by absence of symptoms, but damage to brain has started; it is not possible to recognize the disease in the light of examination at this stage. However, biomarkers can definitely show whether the disease is present.Mild Cognitive Impairment (MCI): The stage was first defined by a researcher, namely Peterson, and it characterized by impaired memory noticed by the patient or relatives, loss in memory or non-memory functions (skills, language, etc.), but the patient can maintain daily life without any problem. The risk of evident dementia in subsequent years is 15 percent for such people. Certain investigators divide this stage into two groups: very mild cognitive impairment and mild cognitive impairment.Alzheimer’s disease is the stage in which symptoms and signs are clearly noticed.
Early-Moderate Stage: It starts with symptoms such as mild dementia, inability remembering certain words and learning new information, fatigue, social withdrawal and depression.Severe - Moderate Stage: The patient’s daily activities are remarkably disrupted. They cannot cook, use utensils, dress up or undress, are unable to go to bathroom or practice personal hygiene or neglects them, cannot find the way to home or confuses rooms in the house.Restlessness and anger, getting lost, loss of motor skills, impairment in social relations and paranoia are very common at this stage.
Advanced and Severely Advanced Dementia: This stage is characterized by total independence of patient to survive. Every patient has a care giver.Physical problems are often faced. Dysfunction in urinary bladder and colon, language impairment or struggle in following simple commands may be accompanied by hallucinations, emotional disorders, loss of environmental awareness and constant wandering. This stage is known to have more pressure on the care giver than the patient. After the stage progresses into very severe stage, the patient becomes bedridden.
The medication used for the disease should be maintained also at this stage.
Although there is no definitive cure for the disease, it is possible to slow down the progression and reduce severity of certain symptoms. Early and accurate diagnosis is crucial with this regard.
Causes
The most critical cause of Alzheimer’s Disease is age. It is one of the most common diseases for individuals above 65 years of age. Gender is another underlying cause of Alzheimer’s disease that is more prevalent in women.
It is because mean life expectancy of females is longer. Low education level, stress, depression, head trauma, other metabolic diseases and genetic factors are among underlying causes of Alzheimer’s disease.
How is Alzheimer’s Disease Recognized?
First sign of Alzheimer’s disease is forgetfulness. Following the first encounter with a doctor, neuropsychiatric tests provide details about presence of the disease, type of dementia and the stage of Alzheimer’s disease. While all these findings may point to evidence regarding the disease, diagnosis of Alzheimer’s may be established more clearly with imaging methods.
How does Alzheimer’s Disease Affect Brain?
The most prominent reason of dementia is the damage to cells and tissues of brain. This damage hinders intercellular communication and thus, brain cannot function properly.
Brain tissues are formed by over 100 billion brain cells which are called neurons. These cells may be affected adversely by numerous intrinsic and extrinsic factors.
Brain tissue consists of independent parts which have unique functions. These areas provide us the ability to think, speak, gain skills, make plans, learn and behave appropriately in social areas.
Damage to cells and tissues of these specific areas leads to gradual deterioration of specific functions. Each type of dementia is caused by involvement of different parts of brain.
For example; Alzheimer’s disease leads to a condition which mostly affects hippocampus, which is also called memory basket, and characterized with accumulation areas (neurofibrillary tangles) in brain cells (neurons) and adverse protein accumulations (amyloid plaques) at intercellular space.
These intra- and inter-cellular adverse accumulations deteriorate cells and intercellular communication as well as atrophy of tissues, resulting in symptoms of the disease.
Atrophy of hippocampus triggers the impaired memory – the first and most critical sign of Alzheimer’s disease.
What Should Be Done to Prevent Alzheimer’s Disease?
Genetic predisposition is the most important risk factor that sets ground for development of Alzheimer’s disease. Family history of Alzheimer's Disease and occurrence of the disease in the age range of 40-60 are suggestive of genetic predisposition.
Incidence rate increases as the age advances. For example; incidence rate doubles in every decade after the age of 65.
Other factors which increase risk of the disease are head trauma, long-term depression, chronic alcohol consumption, hypertension, high cholesterol level and diabetes mellitus.
Is it possible to Prevent Alzheimer’s and What can be done?
Since exact causes of Alzheimer’s Disease are not known, there is no clear evidence about preventive measures. However, some life style modifications may decrease the risk of disease.
To prevent Alzheimer’s Disease;
• Stay physically and mentally active, exercise regularly,
• Keep your blood pressure and blood glucose within normal ranges,
• Increase vegetable and fruit consumption. Prefer a Mediterranean diet.
• Use safety belts and headgear to protect yourselves against head trauma which may occur due to accidents.
• Try to stop or at least limit alcohol consumption, if any; stop smoking.
Who Are In The High-Risk Group?
There are certain conditions that facilitate development of Alzheimer’s disease and they are called risk factors. Known risk factors of Alzheimer’s Disease are as follows:
- Age: Alzheimer’s disease is common in individuals above 65 years of age. The disease is observed in 5% of the population above age of 65, incidence rate increases by 2 folds every 5 year, and the disease may develop in one out of every 2 individual after the age range of 80-85. Nonetheless, recent studies revealed out that the disease starts and progresses without being recognized for two to three decades and diagnosis can be established at the age range of 40-50, if it is investigated.
- Gender: Mean life expectancy of women is longer than men. Considering higher mean life expectancy, higher incidence rate in women is an expected result.
- Depression
- Past History of Diseases: Cardiovascular diseases, hyperlipidemia, diabetes mellitus and thyroid diseases may be considered as risk factors for Alzheimer’s disease.
- History of Head Trauma
- Education: people with low educational level are more predisposed to the disease. Incidence rate of the disease decreases, while educational level increases.
- Heredity and Genetics: 25% of the Alzheimer’s disease cases are genetic and familial in nature. Various genes are identified that are believed to have links with the disease. These genes also ensure formation of neurofibrillary tangles and amyloid plaques which lead to damage to brain and neurons. Overproduction of APOE4 epsilon 4 due to incorrect encoding by Chromosome 19 is an important laboratory test to demonstrate the risk of disease.
- Biomarkers: Some recent laboratory data that enables detection of the Alzheimer’s disease 20 to 30 years before the disease onset support pathological accumulation of proteins in the brain. Abeta 42 and tau proteins can be analyzed in cerebrospinal fluid. These are called bio-markers.
Hospitals
-
 Ataşehir Hospital
Ataşehir Hospital -
 Bakırköy Hospital
Bakırköy Hospital